Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin condition characterized by dry, itchy, and inflamed skin. It is highly prevalent with 15-20% of children and 1-3% of adults in the world affected, and is associated with reduced quality of life, increased health care expenditure, and other atopic diseases such as allergic rhinitis and asthma.1 The pathophysiology of AD is not completely understood, but genetics, skin barrier function, bacterial diversity of skin, and immune dysregulation have all been implicated.2,3
Current treatment of AD depends on the extent and severity of the condition, and should also consider pruritus, sleep disruption, and involvement of sensitive areas such as the face and folds. While powerful systemic agents exist and continue to be developed, treatment of AD relies heavily on topical preparations such as corticosteroids, calcineurin inhibitors, and emollients. Long-term topical corticosteroid use is linked to numerous side effects including skin thinning, telangiectasia, folliculitis, and contact dermatitis.4 Topical calcineurin inhibitors are generally well tolerated, but the FDA has noted concerns about potential links to cancer with a black box warning for these medications.5,6 An even more extensive black box warning adorns the newest non-steroidal topical Janus kinase (JAK) inhibitor, ruxolitinib as well.7 Thus, despite new additions to the therapeutic armamentarium, there is continued demand for alternatives that have decreased risks and side effects.
In recent years, the interplay between immune cells and commensal microbes on the skin has been implicated in AD. Importantly, patients with AD often display decreased microbial diversity.3 Staphylococcus aureus colonization is associated with AD flares and supports the notion that disruption of the normal skin microbiome is implicated in AD.3 This observation has led to a number of research endeavors aimed at investigating the safety and efficacy of probiotics for topical use in AD. Probiotics can be defined as live microorganisms that confer a health benefit.8 Prebiotics, on the other hand, are non-digestible food ingredients that promote growth/activity of the microbiota and thus benefit the host.8 Synbiotics include products with prebiotic and probiotic components in which the prebiotics selectively promote the probiotic bacteria in the same product.8 There are currently several reported and active clinical trials using topical probiotics for AD. The goal of this systematic review is to assess the interventions and data of the clinical trials.
Material and methods
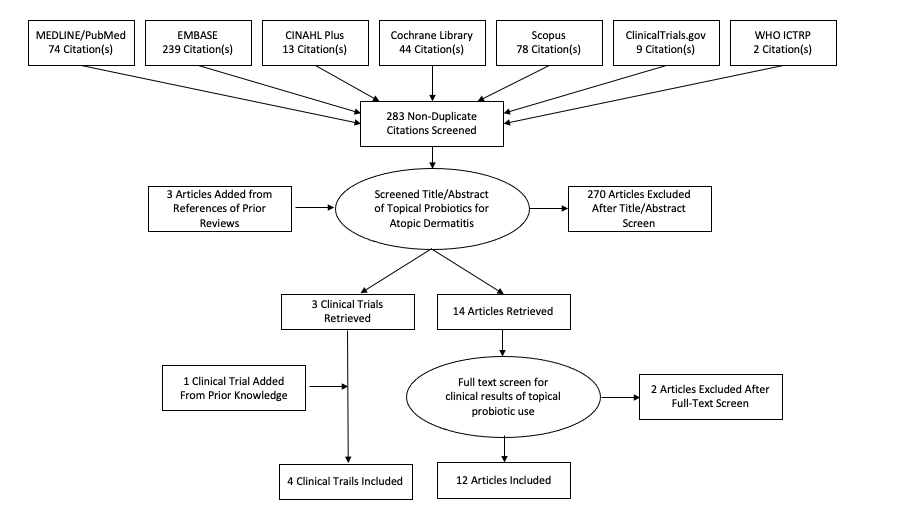
A database search for articles and trials mentioning ‘topical probiotic AND atopic dermatitis’ was developed for the following databases: MEDLINE (PubMed), EMBASE (Embase.com), CINAHL Plus (EBSCO), Cochrane Library (Wiley), Scopus (Elsevier), Clinicaltrials.gov, and the WHO International Clinical Trials Registry Platform from inception on October 17, 2021. All abstracts were reviewed using Rayyan by one author (D.F.) and only those describing the use of topical probiotic in atopic dermatitis were retained (Figure 1). Articles written in languages other than English and poster presentations were excluded from consideration. Three additional studies that did not appear in our literature search were discovered by carefully reviewing the references from prior reviews and one clinical trial was added from prior knowledge. A full text screen was then conducted by one author (D.F.).

Figure 1.Article selection flowsheet detailing uses of topical probiotics for atopic dermatitis in the dermatology literature
Results
There were 9 different bacterial strains used in these interventions: Streptococcus thermophiles, Vitreoscilla filiformis, Lactobacillus sakei, Staphylococus hominis, Staphylococcus epidermidis, Lactobacillus johnsonii, Lactococcus lactis, Roseomonas mucosa, and Lactobacillus reuteri. Vitreoscilla filliformis was the only strain with published results in more than one study. In addition to the one published study assessing Lactobacillus reuteri, a clinical trial is currently recruiting to evaluate the safety and efficacy of Lactobacillus reuteri in children with mild or moderate AD. Of the other clinical trials in progress, one study noted that it would be testing Lactobacillus plantarum. The other noted that it would be testing topically applied Lactobacillus but did not specify the strain.
Common objective clinical measures used to assess improvement in patients included scoring atopic dermatitis (SCORAD) index formula (5 studies), transepidermal water loss (TEWL) (3 studies), or the number of S. aureus colony forming units (2 studies). Subjective tools were also used to evaluate the efficacy of the various treatments.
There were no serious adverse events or treatment complications reported in any of the studies. Findings are summarized in Tables 1 and 2.
Table 1.RCT and open-label trials of topical probiotics
| Citation |
Study type |
Participants recruited |
Intervention |
Treatment duration (dose) |
Outcome measure(s) |
Efficacy |
Adverse effects |
| Di Marizio et al. (2003)9 |
Open-label vehicle-controlled trial |
11 patients; mean age, 20.3±1.8 y (range 18-24 y) |
Application of base cream as vehicle containing S. thermophilus to one forearm and base cream alone to the contralateral forearm |
Twice daily for 2 weeks |
- SCORAD only before treatment
- Pruritus, erythema, and scaling before and after treatment
- Skin ceramide levels
|
- Significant improvement in pruritus (P = 0.000), erythema (P = 0.000), vesiculation (P = 0.000) and scaling (P = 0.003) vs. baseline
- Significant increase in total stratum corneum ceramide level vs. baseline (P = 0.002)
|
No |
| Gueniche et al. (2006)10 |
RCT double blind |
13 patients; mean age, 37.5±16.5 y |
Application of 5% Vitreoscilla filiformis extract containing ointment to one side and vehicle alone to the contralateral side |
Twice daily for 4 weeks |
- mEASI
- EASI
- Pruritus severity index
- Body surface area
|
- Significant improvement in mEASI on the treated side compared to the vehicle side (P = 0,008)
- Significant decrease in EASI index (P = 0.012)
- Significant decrease in pruritus on V. filliformis treated side (P = 0.046)
- No significant difference in pruritus nor body surface area
|
Mild - the most common adverse events were short lasting prickling and burning sensations (23%), likely to be related to the vehicle |
| Gueniche et al. (2008)11 |
RCT double blind |
75 patients; mean age 31 (rage 6-70 year) |
Application of cream containing either 5% V. filiformis lysate (n=37) or vehicle alone (n=38) to predefined areas |
Twice daily for 30 days (5% V. filiformis lysate cream) |
- SCORAD
- Pruritus and sleep loss
- TEWL
- Skin microflora
|
- Significant decrease in SCORAD (P = 0.0044) and pruritus (P = 0.0171) compared with placebo
- Active cream significantly decreased loss of sleep from day 0 to day 29 (P = 0.0171) but between-group difference compared to placebo was not significant (P = 0.21).
- No significant difference between treatment and control groups for TEWL (P = 0.94)
- There was a decline in bacterial colonization but this reduction did not reach a significant level
|
No |
| Park et al. (2014)12 |
RCT double blind |
30 patients recruited, 2 lost to followup; mean age, 14.2 (range 3~37 years) |
Application of L. sakei probio 65-containing emollient to one randomly selected side of the body, and a control emollient to the other side |
Twice daily for 4 weeks |
- IGA
- VAS
- TEWL
- Skin capacitance
|
- No significant difference between treatment and control side for IGA (P = 0.366)
- Significant improvement in VAS (P = 0.006), TEWL (P = 0.007), and skin capacitance (P = 0.001)
|
Mild – 3 patients (11%) experience mild application site reactions which resolved in 3 days |
| Nakatsuji et al. (2017)13 |
RCT double blind |
9 adults; mean age, 28.89±13.61 y; S. aureus carriers |
5 S. aureus culture-positive AD patients were treated with autologous transplant of CoNS clones (S. epidermidis and S. hominis) with antimicrobial activity against S. aureus in cream vehicle base on forearm, vehicle alone was applied to contralateral forearm, 4 patients untreated |
24 hours (1 x 10^5 CFU/cm^2) |
|
- Significant decrease in S. aureus abundance in patients with single application of antimicrobial CoNS strain(s) compared to vehicle (P = 0.0402)
- No significant difference in S. aureus abundance between untreated and vehicle alone patients
|
No |
| Blanchet-Rethore et al. (2017)14 |
Open-label trial |
21 patients; mean age, 33.0 ± 12.5; S. aureus carriers with clinically visible lesions |
Application of heat-treated L. johnsonii lotion on target lesions in place of usual moisturizer, the contralateral lesion was either untreated or treated with the patient's usual moisturizer |
Twice daily, 21±1 day (COS daily moisturizing lotion containing HT La1 at 0.3% w/w) |
- SCORAD
-
S. aureus CFU
- Lesional microbiome analysis
|
- Significant decrease in S. aureus load of treated target lesion comparted with contralateral lesions not treated with HT La1 lotion (P < 0.5)
- Noticeable reduction in proportion of the Staphylococcaceae family
- Significant decrease in mean SCORAD values of target lesion (P = 0.012)
|
No |
| Crespo (2017)15 |
Open-label trial |
53 children |
Application of emollient that combines lysate of Lactococcus lactis and ectoin on atopic skin or very dry skin |
Apply at home under the normal conditions of use |
- Cosmetic quality of cream as rated by children’s parents including moisturizing the skin, nourishing the skin, leaving skin soft and smooth, leaving skin more flexible and elastic, providing a sensation of comfort, and improving the general state of the skin
|
- Cosmetic qualities of cream were rated highly by the parents rating satisfied or very satisfied with cosmetic efficacy of: moisturizing the skin (100%); nourishing the skin (100%); leaving skin soft and smooth (100%); leaving skin more flexible and elastic (98%); providing a sensation of comfort (96%); improving the general state of the skin (100%).
- 94% of parents confirmed they were happy with the results
|
No |
| Myles et al. (2018)16 |
Open-label trial |
10 adults; mean age, 41.9 y (range 90-70) and 5 children; mean age, 10.4 y (range 9-14 y) |
Adults: sucrose solutions containing escalating dose of live R. mucosa applied topically to their bilateral antecubital fossae and one additional body surface area of their choice
Children: given enough solution to treat all involved body surface area |
Adults: twice weekly for 6 weeks, followed by a 4-week washout phase
Children: twice weekly for 16 weeks |
- Adults: objective intensity, subjective regional pruritus, antecubital specific SCORAD, steroid-sparing effects
- Children: worsening SCORAD, worsening itching
|
- Treatment of the hands was not associated with clinical benefit
- Both groups showed significant decrease in mean SCORAD values (P < 0.01 in adults and P < 0.05 in children)
- Significant decrease in subjective pruritus (P < 0.01)
- Significant decrease in topical steroid application (P < 0.05, 2 adults discontinued additional steroid usage)
- In pediatric cohort, significant decrease in ratio of S. aureus to CoNS from the antecubital fossa (P < 0.005).
|
No |
| Butler et al. (2020)17 |
RCT double blind |
36 patients (2 subjects missed visits; mean 36.9 y (range 18-70 y) |
Application of either Lactobacillus reuteri DSM 17938 (n = 17) ointment or control (n = 17) to affected areas of the whole body |
Twice daily for 8 weeks |
- Cutaneous and cosmetic acceptability
- SCORAD index
- Local SCORAD
|
- There was good cutaneous acceptability and cosmetic acceptability in both the probiotic and control groups
- No significant difference between decrease in SCORAD index or local SCORAD vs. control group, although probiotic did show a greater tendency to reduce SCORAD index
- There was mean reduction of SCORAD index in treatment group from baseline at visit 2 (-28%) and at visit 3 (-46%) (P < 0.001)
- There was mean reduction of SCORAD index in control group from baseline at visit 2 (-32%) and at visit 3 (-39%) (P < 0.001)
- There was mean reduction of local SCORAD in treatment group from baseline at visit 2 (-25%) and at visit 3 (-45%) (P < 0.001)
- There was mean reduction of local SCORAD in control group from baseline at visit 2 (-34%) and at visit 3 (-43%) (P < 0.001)
|
No |
Table 2.Clinical trials on topical probiotics planned, in progress, or completed and not yet published in a journal
| Study Title |
Study type |
Number of patients (actual or estimated) |
Study number |
Recruitment status |
| Study of the Skin Microbiome and the Potential of a Topical Probiotic Cream for Atopic Dermatitis18 |
RCT double blind |
40 |
NCT04771910 |
Recruiting |
| Topical L. Reuteri in Children With Atopic Dermatitis (ADreuteri)19 |
RCT double blind |
102 |
NCT04265716 |
Recruiting |
| B244 Topical Spray for the Treatment of Pruritus in Adults With a History of Atopic Dermatitis20 (Nitrosomonas eutropha) |
RCT double blind |
576 |
NCT04490109 |
Recruiting |
| The Effect of Probiotic cream containing bacteria killed in children with Atopic Dermatitis21 |
RCT double blind |
60 |
IRCT20200117046164N1 |
Pending |
Discussion
Manipulating the microbiome in AD clearly has potential to be a novel approach to therapy. While there are many potential ways to achieve this goal, topical application of viable probiotics has substantial evidence of a clinical effect, though there are many unanswered questions and much work remains to be done.
While the results of these studies are promising, there are a few potential confounders and limitations to note. First, some studies allowed concomitant treatment with other active agents including topical corticosteroids, antihistamines, omega-3 fatty acids, and calcineurin inhibitors. This can lead to enhancing the placebo group response, especially in more mild cases, and also may affect the microbiome more directly in ways that are not yet elucidated.
Additionally, there is significant heterogeneity between study designs and endpoints. Design ranged anywhere from a one-time transplant to a 16-week treatment course. Some studies used more objective endpoint measurements including SCORAD and TEWL while others used more subjective endpoints such as parental ratings. Thus, while each of the studies showed some benefit, there is minimal ability to compare the results. Moreover, in nine completed studies, eight different probiotic strains were tested. The variety in agents used leads to a lack of meaningful reproducibility between studies. As such, while the results of each individual study point to a promising role for probiotics in AD management, they cannot be used to support each other.
In addition to problems with drawing comparisons between studies, the study designs implemented also pose issues when extrapolating the results to a larger population. Specifically, the study performed by Crespo testing Lactococcus Lactis used exclusively subjective ratings by parents about the cosmetic efficacy of the emollient. The subjective nature of the evaluation severely limits the generalizability of the study.
Overall, these preliminary trials suggest a beneficial effect and a reassuring safety profile for various strains of topical probiotic bacteria. Undoubtedly, further investigation must continue in this area. More studies should be implemented to corroborate the findings thus far.
Funding Sources
No funding sources were secured for this study.
Disclosures
Dr. Lio reports research grants/funding from the National Eczema Association, AOBiome, Regeneron/Sanofi Genzyme, and AbbVie; is on the speaker’s bureau for Regeneron/Sanofi Genzyme, Pfizer, Eli Lilly, LEO, Galderma, and L’Oreal; reports consulting/advisory boards for Almirall, ASLAN Pharmaceuticals, Dermavant, Regeneron/Sanofi Genzyme, Pfizer, LEO Pharmaceuticals, AbbVie, Eli Lilly, Micreos, L’Oreal, Pierre-Fabre, Johnson & Johnson, Level Ex,Unilever, Menlo Therapeutics, Theraplex, IntraDerm, Exeltis, AOBiome, Realm Therapeutics, and Galderma.
The other authors report no conflict of interest.