Introduction
Topical corticosteroids (TCS) are the first-line treatment for a multitude of dermatological conditions, including atopic dermatitis.1 TCS have been shown to improve the quality of life of patients suffering from atopic dermatitis (AD).2,3 However, despite their near-ubiquitous use, TCS are not without side effects, as seen in Table 1.4 Topical steroid withdrawal syndrome (TSWS) is a condition characterized by erythema, burning and/or itching, and several more distinctive features after cessation of topical and/or systemic corticosteroids.5
In order to understand TSWS, it is first necessary to understand the mechanism of action of TCS. The mechanism of action for corticosteroids is multifactorial, but they bind to a nuclear receptor to inhibit pro-inflammatory transcription factors, including nuclear factor-kappa B(NFkB) and nuclear factor of activated T cells (NFAT). The inhibition of these transcription factors leads to a downstream effect of decreasing synthesis and release of prostaglandins, leukotrienes, and inflammatory cytokines via blockade of phospholipase A2.6
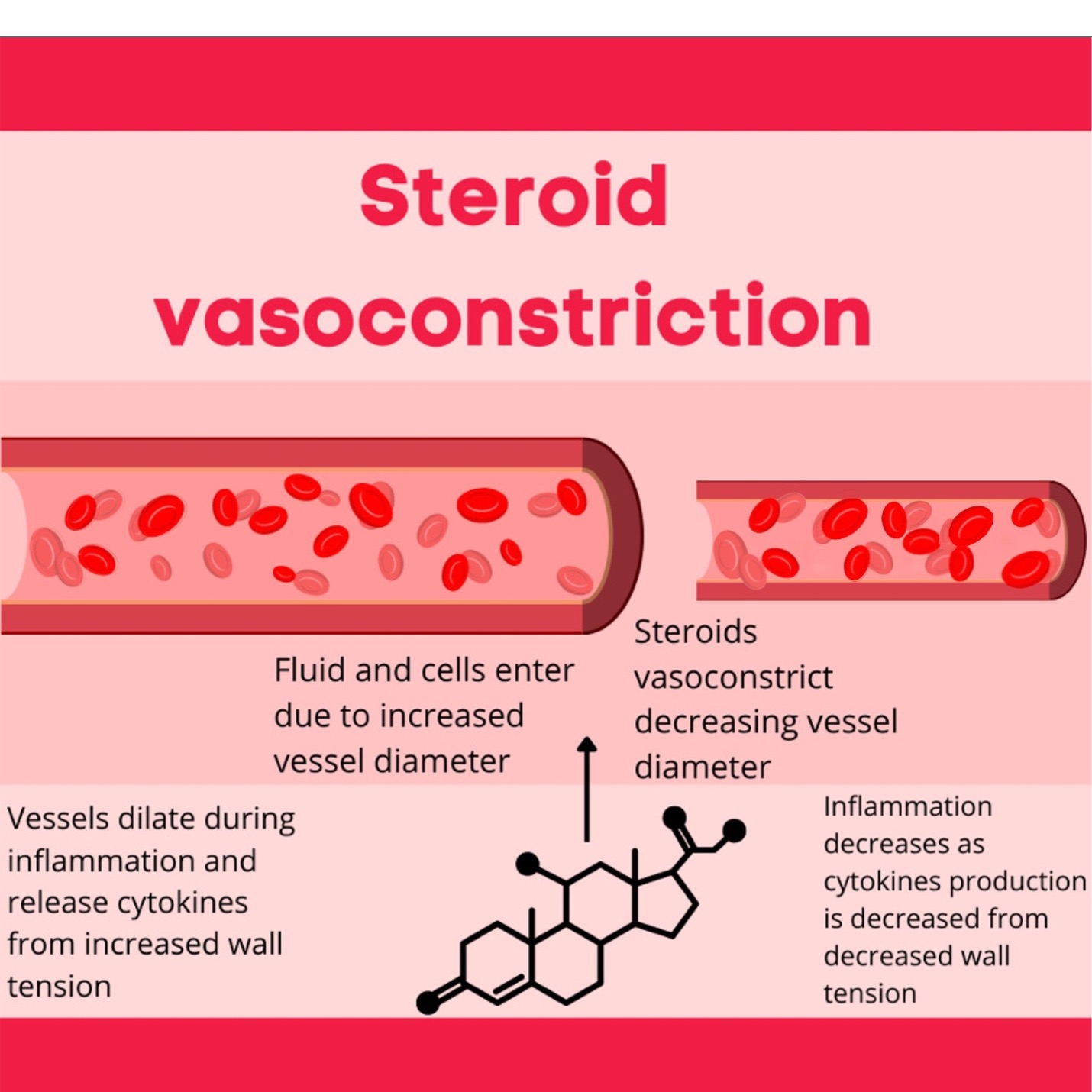
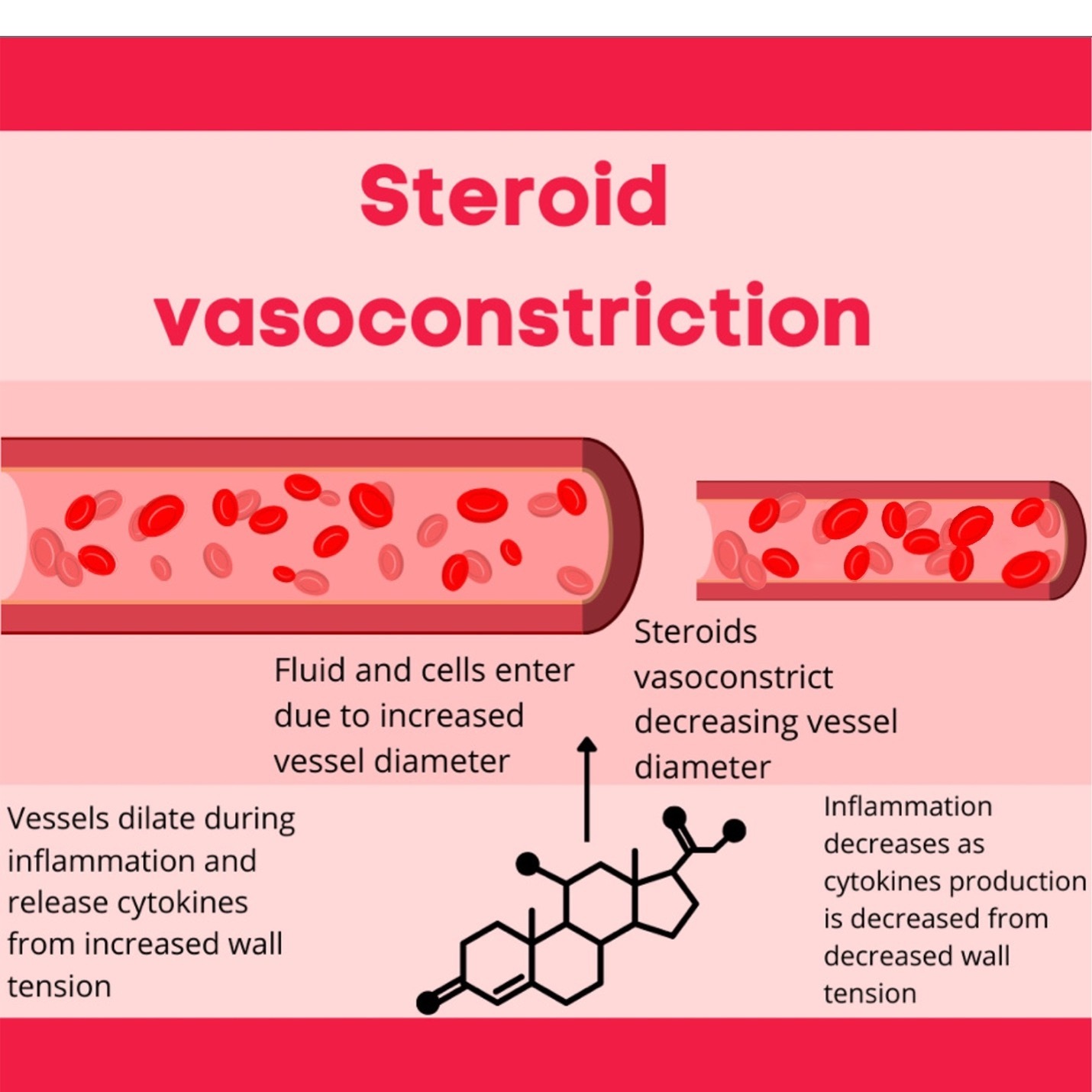
Another important mechanism of action for corticosteroids is their vasoconstrictive effect.7–10 The vasoconstrictive effect correlates with corticosteroids’ anti-inflammatory efficacy. A hallmark of inflammation is vasodilation, either acute or chronic.7–10 When vessels are dilated, they are exposed to increased wall tension and stretch force.7–10 It is precisely this physical stretch of the blood vessel walls and endothelium that has experimentally been shown to result in increased production of proinflammatory cytokines: Vascular endothelial Growth Factor (VEGF), Tumor Necrosis Factor α (TNFα), Monocyte Chemoattractant Protein (MCP-1), Interleukin 6 (IL-6), and Interleukin 8 (IL-8).7–10 Experimentally, increased wall tension can result in opening usually closed gaps in vessel walls.7–10 This opening then leads to fluid and inflammatory cells moving into the surrounding areas.7–10 Thus, when corticosteroids vasoconstrict vessels, there is a decrease in vessel diameter, resulting in decreased wall tension.7–10 The decreased wall tension leads to decreased synthesis of proinflammatory cytokines and decreased movement of fluid and inflammatory cells, thereby decreasing inflammation.7–10 An illustration depicting this mechanism of action can be seen in Figure 1.
Based on the vasoconstrictive effect of topical steroids, there is a hypothesis that posits that TCS decrease the production of nitric oxide (NO), which decreases vasodilation. When TCS are removed, NO levels may increase, leading to rebound vasodilation and erythema.11 Although this seems incomplete given the rest of the clinical presentation of TSWS, it helps explain the often bright red, confluent erythema that reflects another name for this condition: Red Skin Syndrome.12 Additionally, patients with atopic dermatitis may have higher serum baseline levels of NO, possibly offering an explanation for the cause of TSWS in patients with AD. However, this is speculative.13
Another possible pathogenesis for TSWS in patients with AD is barrier dysfunction.13 Patients with AD already have an impaired skin barrier.1 Some studies have suggested that TCS use and subsequent withdrawal leads to barrier disruption.13 More specifically, mouse studies demonstrated that cessation of TCS led to an increase in transepidermal water loss and upregulation of inflammatory cytokines.13 Since patients with AD have pre-existing skin barrier dysfunction, the induction of a cytokine cascade upon TCS cessation could possibly be a mechanism of TSWS in patients with AD.13
TSWS is not yet well-defined, but is typically seen after using a mid- to high-potency TCS in sensitive areas, most often the face and genitals.5,14,15 TSWS appears to occur more commonly in women and historically has been divided into two subtypes: papulopustular and erythroedematous.5,14 However, there is no formal diagnostic criteria and only limited evidence on treatments for TSWS.15
The goal of this retrospective chart review is to closely examine and further characterize key features of TSWS that may be useful for building diagnostic criteria and differentiating it from other important conditions on the differential diagnosis.
Methods
We performed a retrospective chart review of patients seen at a referral-based dermatology clinic focused on AD. The diagnostic code T38.0X5A (“Adverse effect of glucocorticoids”) has been specifically used by the dermatologist (PL) to demarcate the diagnosis of TSWS lacking a more formal code. Topical corticosteroids have numerous potential adverse effects, both locally and systemically, due to their ability to be absorbed. Selected adverse effects are listed in Table 2. Notably, few of these specific adverse effects were identified in this cohort and the diagnostic code was never used for these as each has a more specific code. The diagnosis of TSWS in this series was based on the clinical experience of the dermatologist (PL) as well as available literature. Notably, however, almost every case presented with a self-diagnosis of TSWS. Patient charts were reviewed, and the following variables were collected: age at diagnosis, sex of the patient, location of TSWS skin findings, the severity, and the percent of body surface area covered by TSWS skin findings.
Results
Sixty-nine patient charts were returned after searching for the diagnosis code T38.0X5A. Of this cohort, the average age of diagnosis for TSWS was 35.3 years. TSWS was diagnosed in females with a greater predominance (56/69, 81.16%) than males (13/69, 18.84%). The most common location for TSWS involvement was the anterior neck. TSWS occurred most commonly in patients with severe AD, followed by moderate AD. Additional results are presented in Table 1. The most common types of TCS used included hydrocortisone 2.5%, clobetasol, triamcinolone, desonide, and betamethasone.
Discussion
Similar to previous studies stating that TSWS occurs more often in females, we also found a marked preponderance of TSWS in females.15 Of the 69 patients, TSWS was diagnosed in 7 pediatric patients. Pediatric cases of TSWS appear to be relatively rare, with an estimated 7% of all TSWS cases.16 We found an incidence of 10.1% of pediatric cases in this group. The youngest patient in our cohort was 3 years old, while the oldest patient was 69, exhibiting the broad age range in which TSWS can occur. Contrary to previous studies, we did not see TSWS in the genital region, but we did see it frequently on the face.5,14,15
The overall presentation of TSWS is wide-varying and multifaceted.17 One of our patients presented with perioral dermatitis, consistent with literature stating that discontinuation of topical steroids can lead to rebound flares of perioral dermatitis.18 Additionally, one of our patients presented with angioedema of the lips, similar to a case study of another patient presenting with TSWS and swelling of the lips.19
Two of our patients presented with a recent or concurrent viral skin infection at the time of diagnosis, while two of our patients presented with lymphadenopathy. Literature has described erythema accompanying TCS withdrawal in areas of the body where TCS were never applied.20 This “rebound eruption” can be accompanied by a high fever in severe cases.20 Therefore, in a patient presenting with a widespread erythematous rash with a history of topical steroid use and systemic signs of infection, TSWS could be considered in addition to a bacterial or viral infection.
The differential diagnosis of TSWS should include atopic dermatitis and allergic contact dermatitis as the primary considerations. Nevertheless, a full differential diagnosis, including but not limited to cutaneous T-cell lymphoma, psoriasis, rosacea, and scabies should be considered given the somewhat heterogeneous presentations described.14
While the literature has stated that there is no relation between adrenal fatigue and TSWS, one of our patients had a history of adrenal suppression upon presentation of TSWS.20
While the dermatologist (PL) has clinically diagnosed TSWS, there is no accepted diagnostic criteria nor a standardized International Classification of Disease (ICD) code for TSWS, only an ICD code for the adverse effect of glucocorticoids.21
Unique findings of this study include higher rates of TSWS in children, a lack of TSWS found in the genital region, and a broad age range in which TSWS can present (3 years to 69 years of age).
Limitations of this study include a lack of comprehensive patient notes, thus a lack of complete patient medical history, medication use, and other relevant factors. Furthermore, we could not assess what dosage of topical corticosteroids causes TSWS and how long TSWS lasts due to large variations in time, inconsistent documentation, and lack of follow-up appointments. We could not determine what frequency and duration of TCS application led to TSWS.
Additionally, we could not determine if one type of TCS led to TSWS more than another; this is an area for future study.
Future Directions: While dermatology is typically not a field of highly detailed patient notes in conditions such as TSWS, we recommend dermatologists document a complete and thorough medical history to further add to the literature. Furthermore, we advocate for the use of a TSWS-specific ICD code; the adverse effects of glucocorticoids may be too broad. Additionally, because of the provider mistrust surrounding TSWS, we encourage dermatologists to actively listen to their patients and give special attention to the social issues encompassing TSWS. Especially in pediatric cases, a parent’s steroid phobia can have long-lasting effects on children with severe AD.
In patients with underlying AD and concurrent TSWS, dupilumab, phototherapy, conventional immunosuppressants such as cyclosporine, and topical non-steroidal agents may all potentially be useful in managing the condition. However, given the complexity of the condition and the nuances of each treatment, it is important that a shared decision making approach be undertaken to optimize care.
Conclusion
We describe 69 patients in our retrospective chart review with TSWS. For our cohort, the average age of presentation with TSWS was 35, more commonly occurred in females, most frequently occurred on the anterior neck, and occurred in patients with severe AD. One of the most challenging aspects of TSWS is the breakdown of the relationship between the dermatologist and patient.20,22 Alarmingly, most cases of TSWS are self-diagnosed due to a lack of a diagnostic consensus for TSWS.17 Mistrust and lack of faith in the provider can lead to a lack of adherence, follow-up appointments, and potentially worsening symptoms. After being prescribed steroids multiple times, many patients presume that their dermatologist does not know how to treat their condition and is not hearing their concerns.20
Many patients have turned to alternative and complementary medicine and formed online support groups for TSWS, underscoring the need for better diagnostic and treatment information for dermatologists.19 Dermatologists may incorporate integrative treatment modalities in addition to conventional medicine to provide the best possible care. Perhaps the incorporation of integrative care in addition to conventional medicine may increase patient-provider trust and strengthen the doctor-patient relationship.
Due to the frequency that TCS are prescribed, it is important for prescribers to closely monitor the strength, dosage, and frequency of use by their patients.1,5,14,15
Without clinical acceptance of this diagnostic entity or even basic criteria for diagnosis, further developments in understanding the pathogenesis of the disease, let alone developing treatments, will be stymied. Thus, for now, it is imperative to focus efforts on prevention by leveraging non-steroidal alternatives when overuse is suspected.
Funding Sources
No funding sources were secured for this study.
Disclosures
Dr. Lio reports research grants/funding from AbbVie, AOBiome, and Regeneron/Sanofi Genzyme; is on the speaker’s bureau for AbbVie, Eli Lilly, Galderma, Hyphens, Incyte, LEO Pharma, L’Oreal, MyOR Diagnostics, ParentMD, Pfizer, and Regeneron/Sanofi Genzyme; and reports consulting/advisory boards for AbbVie, Almirall, Amyris, AOBiome, Arbonne, ASLAN Pharmaceuticals, Burt’s Bees, Castle Biosciences, Codex Labs, Concerto Biosciences (stock options), Dermavant, Eli Lilly, Exeltis, Galderma, IntraDerm, Johnson & Johnson, LEO Pharma, L’Oreal, Menlo Therapeutics, Micreos (stock options), Pfizer, Pierre-Fabre, Regeneron/Sanofi Genzyme, Theraplex, and Unilever. In addition, Dr. Lio has a patent pending for a Theraplex product with royalties paid, and is a Board member and Scientific Advisory Committee Member of the National Eczema Association.
KA reports no conflict of interest.